Hip pain treatment is not a single decision — it’s a spectrum of options, each matched to a specific stage, cause, and severity of your condition. Whether you’re managing early hip discomfort from an active lifestyle or living with the grinding daily pain of advanced osteoarthritis, there is a clear, evidence-based path from where you are now to where you want to be.
This guide walks through the full range of hip pain treatment options available at City Orthopaedics Sports Medicine — from the first conservative steps to total hip replacement — with expert insight from Dr. Oladapo M. Babatunde, MD, FAAOS, one of New Jersey and New York’s most trusted orthopedic surgeons.
Understanding Hip Pain: Why It Happens and Who It Affects
Hip pain is one of the most common musculoskeletal complaints seen by orthopedic specialists — affecting athletes in their twenties and retirees in their seventies for very different reasons. The hip is a ball-and-socket joint that bears the full weight of your upper body during every step you take. That combination of load and motion makes it vulnerable to a wide range of conditions.
The location of your pain often points to the underlying cause:
- Groin pain typically signals a problem inside the hip joint itself — arthritis, labral tear, or hip impingement
- Outer hip or buttock pain often points to bursitis, IT band syndrome, or piriformis syndrome
- Pain radiating down the leg may suggest nerve involvement from the lower back rather than the hip joint itself
- Deep aching pain that worsens at night is a common feature of hip osteoarthritis
Getting the diagnosis right is the essential first step. Treating the wrong cause of hip pain — even with the right treatment — produces no improvement.
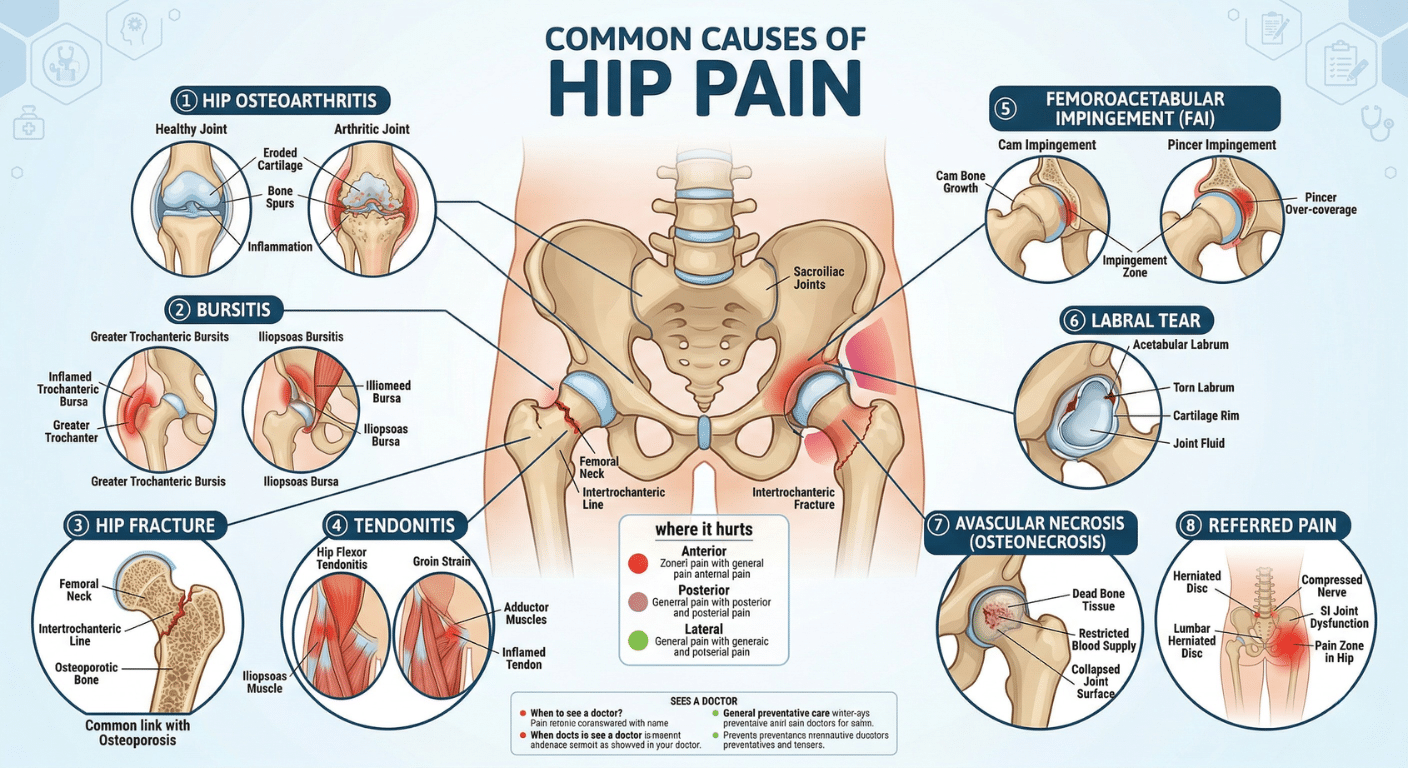
Common Causes of Hip Pain We Treat
At City Orthopaedics Sports Medicine, our hip pain patients present with a wide variety of underlying conditions. The most frequently diagnosed include:
- Hip osteoarthritis — progressive wearing of the cartilage that cushions the joint, most common in adults over 50 but also seen in younger patients with prior injury
- Hip labral tears — damage to the ring of cartilage (labrum) that lines the hip socket, common in athletes and active adults
- Femoroacetabular impingement (FAI) — abnormal contact between the ball and socket of the hip, often causing pain with deep flexion or twisting
- Trochanteric bursitis — inflammation of the bursa sac on the outer hip, producing sharp or burning lateral hip pain
- Hip flexor tendonitis or strain — overuse or acute injury of the hip flexor muscles, frequent in runners and cyclists
- Avascular necrosis (osteonecrosis) — loss of blood supply to the femoral head, leading to bone collapse if untreated
- Hip fractures — most common in older adults following a fall, requiring urgent evaluation
How Hip Pain Is Diagnosed at City Orthopaedics
An accurate diagnosis is the foundation of every effective hip pain treatment plan. At City Orthopaedics, the diagnostic process is thorough, structured, and patient-centered.
Your evaluation typically includes:
- Detailed history — when the pain started, what activities aggravate or relieve it, prior injuries, and how it’s affecting daily function
- Physical examination — range of motion testing, provocative maneuvers to identify labral or impingement pathology, gait assessment, and strength evaluation
- Imaging review — X-rays to assess joint space, bone alignment, and arthritis severity; MRI for soft tissue evaluation (labrum, tendons, cartilage); CT scan when precise bony anatomy is needed
“The most important thing we can do for a hip pain patient is listen carefully and examine thoroughly before any imaging,” says Dr. Babatunde. “The clinical story tells us what we’re looking for — imaging confirms it. That sequence matters.”
Conservative Hip Pain Treatment Options
The overwhelming majority of hip pain patients do not need surgery, at least not initially. City Orthopaedics’ approach is always conservative-first — exploring every non-surgical option before a surgical recommendation is ever made.
Physical Therapy and Targeted Exercise
Physical therapy is the cornerstone of non-surgical hip pain treatment. A well-designed rehab program addresses the specific muscular imbalances and movement patterns that are loading the hip abnormally. For most hip conditions, this includes:
- Hip flexor and iliopsoas stretching and strengthening
- Glute and hip abductor strengthening to stabilize the pelvis
- Core strengthening to reduce load transfer to the hip joint
- Gait retraining and movement pattern correction
- Low-impact aerobic conditioning — cycling, swimming, and aqua therapy
Activity Modification
Continuing high-impact activity through a flare-up can accelerate joint damage. Temporary modification — switching from running to cycling, reducing mileage, or adjusting technique — often provides enough unloading for the hip to calm down and begin healing. This is not “stopping activity forever.” It’s a strategic reduction that protects long-term function.
Medications
Anti-inflammatory medications (NSAIDs) are frequently used to reduce hip joint inflammation and pain. These may be appropriate for short-term management of bursitis, tendonitis, or early arthritis flare-ups. Longer-term use requires physician oversight due to gastrointestinal and cardiovascular considerations.
Corticosteroid Injections
Corticosteroid (cortisone) injections deliver powerful anti-inflammatory medication directly into the hip joint or surrounding bursae. They are particularly effective for bursitis and moderate osteoarthritis, providing weeks to months of pain relief that allows patients to engage more productively in physical therapy and daily function.
Hyaluronic Acid (Viscosupplementation) Injections
For hip osteoarthritis specifically, hyaluronic acid injections supplement the joint’s natural lubricating fluid. While results vary by patient, many experience meaningful pain reduction and improved mobility — particularly those who are not yet candidates for or interested in joint replacement.
Platelet-Rich Plasma (PRP)
PRP therapy uses concentrated growth factors from the patient’s own blood to support tissue healing and reduce inflammation. It is increasingly used for labral tears, tendonitis, and early cartilage degeneration in patients seeking regenerative options before committing to surgery.
When Conservative Care Is Not Enough
Non-surgical treatment is effective for a significant portion of hip pain patients. But there are clinical situations where conservative care reaches its limit — and continuing to delay surgical intervention makes outcomes worse, not better.
Surgical evaluation is typically appropriate when:
- Conservative treatment has been consistently applied for 3–6 months without adequate relief
- Imaging reveals structural damage — a labral tear, advanced cartilage loss, or femoral head collapse — that cannot heal on its own
- Hip pain is significantly limiting your ability to work, sleep, or perform basic daily activities
- You are relying on escalating doses of pain medication to function
- Joint instability or mechanical symptoms (locking, catching) suggest structural failure
“My role at that point is to make sure the patient fully understands their options and has realistic expectations about what surgery can and can’t achieve,” says Dr. Babatunde. “A well-timed surgical decision, with full patient understanding, produces far better outcomes than a delayed or pressured one.”
Surgical Hip Pain Treatment Options
Hip Arthroscopy
Hip arthroscopy is a minimally invasive procedure that uses a small camera and instruments inserted through tiny incisions to address problems inside the hip joint without opening it fully. It is the preferred surgical approach for:
- Labral tears — repair or reconstruction of the damaged labrum
- Femoroacetabular impingement — reshaping the abnormal bone that’s causing painful contact
- Removal of loose bodies within the joint
- Early cartilage damage
Recovery from hip arthroscopy is significantly shorter than from open procedures — most patients return to light activity within 6–8 weeks, with full sport or high-demand activity clearance typically at 4–6 months.
Hip Osteotomy
An osteotomy involves surgically reshaping the bones of the hip to correct alignment and redistribute load away from damaged cartilage. It is typically recommended for younger patients with structural hip dysplasia or FAI who have meaningful remaining cartilage — essentially buying time and preserving the natural joint before replacement becomes necessary.
Partial Hip Replacement (Hemiarthroplasty)
In cases where only one component of the joint is damaged — most commonly the femoral head following a fracture — a partial hip replacement replaces only the ball portion of the joint while preserving the natural socket. This is most frequently performed in older patients following hip fractures.
Total Hip Replacement (Total Hip Arthroplasty)
Total hip replacement is one of the most successful elective procedures in all of medicine — with patient satisfaction rates consistently above 90%. It involves replacing both the damaged femoral head (ball) and the acetabulum (socket) with precision-engineered implants made of metal, ceramic, and high-grade polyethylene.
Total hip replacement is most appropriate for:
- Advanced hip osteoarthritis that has not responded to conservative care
- Avascular necrosis with significant femoral head collapse
- Post-traumatic arthritis following prior hip injury or fracture
- Inflammatory arthritis (rheumatoid or other) causing severe joint destruction
Most patients are walking with assistance the day of or after surgery. Full functional recovery — including return to low-impact activity — typically occurs within 3–6 months. Modern implants are designed to last 20–30 years with appropriate activity levels.

Hip Replacement Recovery: What to Expect
Recovery from total hip replacement at City Orthopaedics is structured, supported, and closely monitored. Dr. Babatunde provides detailed post-operative protocols and personally monitors each patient’s progress through milestones.
Typical recovery timeline:
- Day 1–2: Walking with assistance; physical therapist begins mobilization
- Week 1–3: Home with walking aid; home exercise program begins
- Week 4–6: Most patients transition off walking aids for flat surfaces
- Month 2–3: Formal outpatient physical therapy progresses strength and gait
- Month 3–6: Return to driving, light activity, and most daily tasks
- Month 6–12: Full benefit of the replacement typically realized; cleared for low-impact recreational activity
Patients are strongly advised against high-impact activities like running and jumping post-replacement — not because they can’t be active, but because protecting the implant extends its lifespan significantly.
Why Choose City Orthopaedics for Hip Pain Treatment in NJ and NY
Dr. Oladapo M. Babatunde, MD, FAAOS is a fellowship-trained, board-certified orthopedic surgeon and Fellow of the American Academy of Orthopaedic Surgeons with deep expertise in hip pathology — from sports-related labral injuries in young athletes to total hip replacement in older adults with advanced arthritis.
Patients consistently describe Dr. Babatunde as thorough, accessible, and genuinely invested in their outcomes — a surgeon who takes time to explain every option, answer every question, and build a treatment plan around the patient’s goals, not a standard protocol.
City Orthopaedics serves hip pain patients across:
- East Rutherford, NJ — Primary hub for Bergen County and North Jersey patients
- Paramus, NJ — Convenient access across Bergen County
- West Orange, NJ — Serving Essex County and surrounding communities
No referral is required to schedule. Most major insurance plans are accepted. Same-week appointments are available for acute hip pain and urgent evaluations.
If hip pain is limiting what you can do — at work, in sport, or in daily life — the right hip pain treatment plan starts with the right evaluation. Book an appointment with Dr. Babatunde at City Orthopaedics Sports Medicine today and take the first step toward lasting relief.
Frequently Asked Questions About Hip Pain Treatment
How do I know if my hip pain needs surgery?
Surgery is typically considered when conservative treatments — physical therapy, injections, and activity modification — have been consistently applied for 3–6 months without adequate relief, or when imaging reveals structural damage that cannot heal on its own. Dr. Babatunde evaluates each patient individually and presents all available options with honest, objective guidance before any surgical recommendation is made.
What is the fastest way to relieve hip pain without surgery?
The most effective non-surgical approach combines targeted physical therapy to correct muscle imbalances, activity modification to reduce joint load, anti-inflammatory medication for acute flare-ups, and corticosteroid or hyaluronic acid injections when appropriate. The fastest results typically come from starting PT early and pairing it with physician-guided medication management.
What is the difference between hip arthroscopy and hip replacement?
Hip arthroscopy is a minimally invasive procedure that repairs or treats problems inside the hip joint — such as labral tears or impingement — while preserving the natural joint. Total hip replacement removes and replaces the damaged joint surfaces with artificial implants. Arthroscopy is appropriate for younger patients with specific structural problems; replacement is typically reserved for advanced arthritis or severe joint damage.
How long does hip replacement surgery last?
Modern total hip replacement implants are designed to last 20–30 years, depending on the patient’s activity level, weight, and implant type. Younger or more active patients may eventually require a revision procedure. Advances in implant materials — including ceramic-on-polyethylene and highly cross-linked components — continue to improve long-term durability.
Can hip osteoarthritis be treated without hip replacement?
Yes — many patients with hip osteoarthritis are successfully managed non-surgically for years with physical therapy, weight management, low-impact exercise, and injectable treatments. However, when cartilage damage is severe and conservative care no longer provides adequate function or pain relief, total hip replacement offers the most durable and predictable long-term outcome.
Where can I get expert hip pain treatment in New Jersey or New York?
City Orthopaedics Sports Medicine offers comprehensive hip pain treatment — from conservative care through total hip replacement — at offices in East Rutherford, Paramus, and West Orange, NJ, and Manhattan, NY. Dr. Oladapo M. Babatunde, MD, FAAOS, leads hip care across all locations. Book your appointment online here.